What Is Bronchopulmonary Dysplasia?
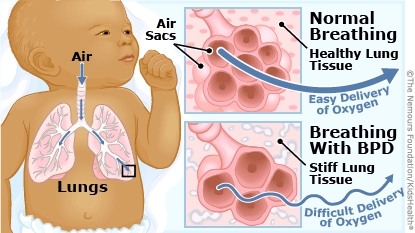
Bronchopulmonary dysplasia (BPD), sometimes called chronic lung disease, is a problem with how a baby’s lung tissue develops.
Babies who are born very early or who have breathing problems after birth are at risk for bronchopulmonary dysplasia (brahn-ko-PUL-moh-nair-ee dis-PLAY-zhee-uh). Most infants get better with few long-term health problems, but some need intensive medical care.
What Happens in Bronchopulmonary Dysplasia?
Babies aren’t born with the condition. It happens when a baby has been on oxygen or on a breathing machine for a long time. This can damage the lungs, causing inflammation (swelling and irritation) and scarring. As a result, the lungs do not develop as they should. It’s more common in premature babies.
Mechanical ventilators do the breathing for babies whose lungs are too immature to let them breathe on their own. Oxygen gets to their lungs through a tube inserted into the baby’s trachea (windpipe). The machine uses pressure to move air into the baby’s stiff, underdeveloped lungs. Many babies do not need a breathing tube, but still need extra oxygen and pressure. Doctors use nasal prongs to send the oxygen and pressure into the baby’s lungs.
These babies need oxygen in a higher concentration than what’s in the air we breathe. Over time, the pressure from the ventilation and extra oxygen intake can injure a newborn’s delicate lungs. This kind of long-term injury prevents normal lung development. So these babies continue to have problems with breathing and need extra oxygen sent to their lungs. Premature babies who need oxygen therapy for more than 28 days are considered to have bronchopulmonary dysplasia.
Sometimes, bronchopulmonary dysplasia can happen if another problem affects a newborn’s lungs, such as birth defects, heart disease, pneumonia, and other infections. These can cause the inflammation and scarring of BPD, even in a full-term newborns.
How Is Bronchopulmonary Dysplasia Diagnosed?
To diagnose BPD, doctors consider:
- how early a baby was born
- how long the baby gets oxygen therapy
- the oxygen levels the baby gets
- the pressure levels the baby gets to flow air into the lungs
Chest X-rays and an echocardiogram also can help doctors look for the condition and see how severe it is.
How Is Bronchopulmonary Dysplasia Treated?
No medical treatment can cure bronchopulmonary dysplasia right away. Treatment focuses on giving the baby good nutrition to help the lungs grow and develop.
During this time, babies get breathing and oxygen help so that they can grow and thrive. With good nutrition and care, many babies can come off oxygen and breathe on their own. Babies get intense care in the hospital, usually in a neonatal intensive care unit (NICU), until they can breathe well on their own, without a mechanical ventilator.
Some babies may get high-frequency ventilation. This continuous low-pressure ventilation helps reduce the lung damage. Not all hospitals have this option, but some with large NICUs do.
Medicines
Doctors sometimes use different medicines to help a baby’s lungs work better. These include:
- bronchodilators (such as albuterol) to help keep the airways open
- diuretics (such as furosemide) to reduce fluid buildup in the lungs
- inhaled steroids (such as budesonide) to ease inflammation in the lungs
A baby with severe BPD might get a short course of steroids given into the stomach or into the blood. This strong anti-inflammation medicine has some serious short-term and long-term side effects. Doctors only use it after talking with a baby’s parents so they understand its potential benefits and risks.
A baby might get antibiotics to fight bacterial infections. That’s because babies with BPD are more likely to develop pneumonia.
A baby’s treatment also might include getting a surfactant. This a natural lubricant that improves breathing.
Feeding Help
Babies who need care in a hospital for bronchopulmonary dysplasia may need feedings of high-calorie formulas through a gastrostomy tube (G-tube). This tube is inserted through the belly to deliver nutrition right to the stomach. This helps babies get enough calories to grow.
In severe cases, babies with BPD can’t use their gastrointestinal systems to digest food. They need intravenous (IV) feedings called parenteral nutrition . These feedings provide fats, proteins, sugars, and nutrients through a small tube inserted into a large vein through the baby’s skin.
Infants with BPD might need care in the NICU for several weeks to a few months. After leaving the hospital, some might still need continued medicine, breathing treatments, or even oxygen at home.
Most babies are weaned from extra oxygen by the end of their first year. A few may need breathing help from a ventilator for several years. Rarely, some need that help throughout life. In those cases, the baby will need a tracheostomy (or “trach”) tube. Doctors insert this plastic tube into the windpipe by making a small hole (called a stoma) in the baby’s neck.
It takes time for babies with bronchopulmonary dysplasia to get better. Many will recover close to normal lung function. But scarred, stiffened lung tissue won’t always work as well as it should. As infants grow, new healthy lung tissue can form and grow, and might take over much of the work of breathing for damaged lung tissue.
What Problems Can Happen?
After getting better, some infants might have long-term problems from bronchopulmonary dysplasia. They’re at risk for respiratory infections, such as the flu, respiratory syncytial virus (RSV), and pneumonia. If they get an infection, they tend to get sicker than most children do. Babies with BPD may continue to have episodes of wheezing and well into childhood.
BPD sometimes causes fluid buildup in the lungs, known as pulmonary edema. This makes it harder for air to move through the airways. Diuretics can prevent fluid buildup, but also have some side effects, such as:
- dehydration
- kidney stones
- hearing problems
- low potassium, sodium, and calcium levels
Infants with BPD often grow more slowly than other babies, have problems gaining weight, and tend to lose weight when they’re sick.
How Can Parents Help?
Parents play a big role in their baby’s care. A baby with BPD is at risk for respiratory infections. So it’s important to:
- Limit visits from people who are sick.
- Choose a small childcare center, if needed, so there’s less exposure to sick kids.
- Make sure your baby gets all recommended vaccinations.
- Keep your child away from tobacco smoke, including secondhand smoke.
If your baby gets oxygen at home, the doctors will show you how to work the tube and check oxygen levels.
Some children may need bronchodilators to relieve asthma-like flare-ups. You can give this medicine to your child with a puffer or nebulizer, which produces a fine spray of medicine that your child then breathes in.
A baby who has trouble growing might need a high-calorie formula. Formula feedings may be given alone or along with breastfeeding. Sometimes, babies with BPD who are slower to gain weight will go home from the NICU on G-tube feedings.
When Should I Call the Doctor?
When your baby comes home from the hospital, watch for signs of breathing problems.
Call your doctor or get medical care right away if your baby:
- is breathing faster than normal
- is working much harder than usual to breathe:
- the belly sinks in with breathing
- the skin between the ribs pulls in with each breath
- gets tired or lethargic from working to breathe
- coughs more than usual
- is panting or grunting
- is wheezing
- has pale, darker, or bluish skin around the lips or fingernails
- has trouble feeding or is spitting up a lot or vomiting up feedings
